
- Stem cell therapy is an innovative approach that uses healthy cells to replace those lost due to disease.
- Rejection from the body’s immune system, however, presents a major challenge.
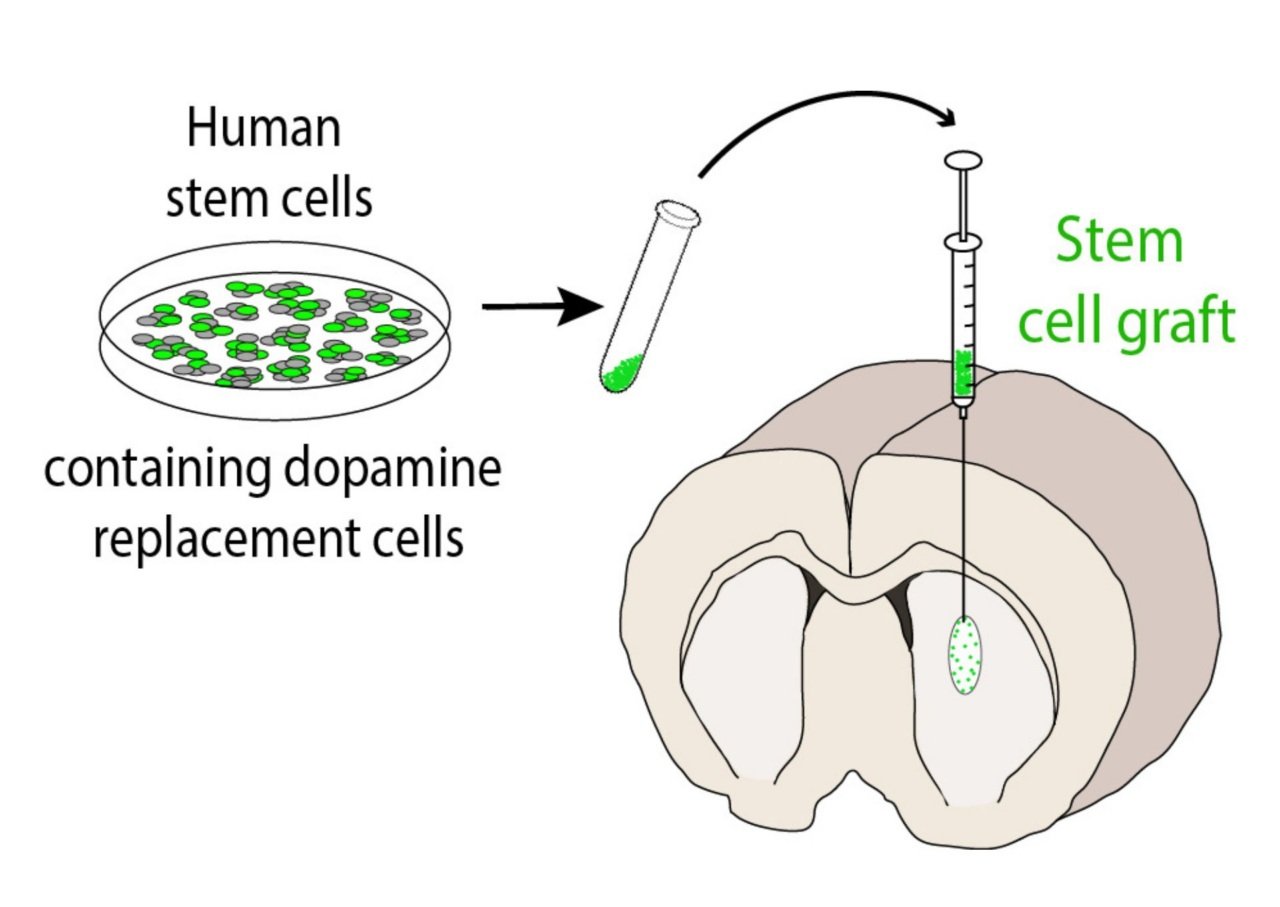
- Florey researchers are working on therapies which involve the transplantation of dopamine-releasing neurons with the potential to repair brain damage caused by Parkinson’s disease. The transplanted cells are engineered to evade immune system detection.
Every human body is made up of trillions of cells — tiny building blocks that work together to keep us healthy and alive. When disease strikes, these cells can be badly damaged or even lost altogether.
Stem cell therapy is an innovative approach to medicine that uses healthy cells to replace those lost due to disease. Instead of focusing on managing a patient’s symptoms, cell therapy aims to alter the course of the disease by stopping its progression and reversing the damage caused.
By replacing lost cells, the aim is to restore activity in a specific tissue or organ.
In the case of Parkinson’s, the hope is to replace dopamine-producing brain cells that die as the disease progresses and to bring back lost movement and brain function.
How stem cells are created
So, where do we get these cells from?
Specialist labs typically grow stem cells from donated blood or skin cells. These lab-grown cells can then be turned into almost any cell type in the human body. These stem cells are known as induced pluripotent stem cells (iPSCs).
In our Parkinson’s lab at The Florey, we specifically guide these stem cells to develop into dopamine-producing neurons. We then use these cells as a source for transplantation therapy in animal models of Parkinson’s disease, where we can observe recovery of motor deficits.
In the clinic, replacement cells often come from healthy donors and can be used in multiple patients. This is a “one-for-many” approach, referred to as allogeneic therapy.
Donor-derived cells are specially modified to become what are known as precursor cells, which can then be developed into the specific cell types needed for transplantation.
A second approach involves taking cells directly from the patient, modifying them, and then reintroducing them into the same patient. This is a “one-for-one” approach, known as autologous therapy.
However, this method is much more expensive and requires extensive oversight for each recipient. Moreover, the patient’s own cells may still carry disease-causing mutations, which can limit the therapy’s effectiveness. For these reasons, the first approach is often preferable.
Immune rejection
While allogeneic therapy is preferred, it does present a major challenge: immune rejection.
Because the transplanted cells are not the patient’s own, the body may treat them as being foreign, causing them to be rejected by the recipient’s immune system.
During my PhD, I investigated strategies to overcome this issue by effectively providing transplanted cells with an “invisibility cloak”. Although these cells are allogeneic, this modification helps them evade detection by the recipient’s immune system by hiding in plain sight, reducing the likelihood of rejection.
We are now working toward translating these cloaked stem cells into clinical applications.
While the focus of my research has been Parkinson’s disease, cloak technology could be used for treating other diseases for which cell-based therapies are a viable option, such as stroke, Huntington’s disease, heart diseases and diabetes.
